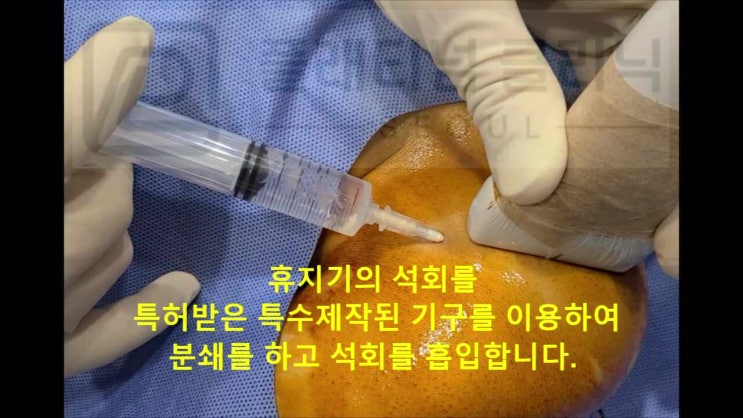
Hello. I am Dr. Dongkyu Lee, an orthopedic specialist. It has been a while since I last wrote. I have been busy with various preparations, so I am only getting to write now. Many people suffer from calcific tendinitis. But those who have received treatment from me no longer suffer from calcific tendinitis. That is because there is a way to resolve calcification in one session. "Calcific Deposit Aspiration" - this is a procedure I developed and named over more than 10 years of work. I have filed a patent for the instruments used. It is a procedure that uses specially manufactured guides and drills to crush and aspirate the calcification. Calcific deposit aspiration requires anesthesia. Simple local anesthesia causes too much pain for the patient, so I perform a brachial plexus nerve block to completely control shoulder pain before proceeding. I remember a patient with excruciating pain from shoulder calcific tendinitis who, after receiving the brachial plexus block, said that just being pain-free like this was enough to feel alive. In the early days, I performed the procedure with only simple local anesthesia, and I remember a patient who cried through the entire procedure. That is why I now use the brachial plexus nerve block to minimize or completely eliminate pain during the procedure. I have always worried about this during surgeries too - of course procedures and surgeries cause significant pain, and I have constantly thought about how to minimize it. The brachial plexus nerve block is not general anesthesia but is a comparable level of anesthesia that requires medical staff to closely monitor the patient's condition, so hospitalization is necessary. After sufficient observation and confirmed stability, same-day discharge is possible, and overnight stays are arranged when needed. After anesthesia, the specially manufactured instrument (guide, patent pending) is inserted into the calcification, and the specially manufactured instrument (calcification-crushing drill bit) is used to crush the calcification.
As shown in the video, the calcification is crushed using the specially manufactured guide and drill.
After crushing the calcification, the crushed material is flushed out using saline solution.

Many patients ask: Can all calcifications be removed? They have been told that depending on the stage of calcification, the properties differ and removal may not be possible, and so on.
Calcific deposit aspiration can remove calcification at any stage of calcific tendinitis. (With the right specialized instruments and expertise, 99% of calcifications can be removed.) Dr. Dongkyu Lee
Calcific tendinitis progresses through 3 stages: formative, resting, and resorptive. In the formative and resting stages, the calcification is hard, so it absolutely cannot be removed by simply aspirating with a syringe. Some patients have told me: "At another hospital, they tried to aspirate with a syringe but nothing came out." "They said the calcification is too hard, so they could only manage pain with steroid injections and try shockwave therapy." I hear these stories frequently. The calcific deposit aspiration procedure I developed directly crushes the calcification using specially manufactured instruments (guide and drill), then aspirates it. This is why even hard formative and resting-stage calcifications can be removed. Resorptive-stage calcification has a paste-like consistency. Some of it can be aspirated with a syringe, but because of its sticky nature, it clings to the inside of the tendon, making complete removal impossible through simple aspiration alone. Calcific deposit aspiration addresses these sticky calcifications too, by minimizing tendon damage while crushing and aspirating the residual calcification, making complete removal possible even in the resorptive stage. Let me walk you through examples of each stage. First, let us look at a formative-stage case, where aspiration was said to be impossible. Here is a formative-stage calcific tendinitis case.

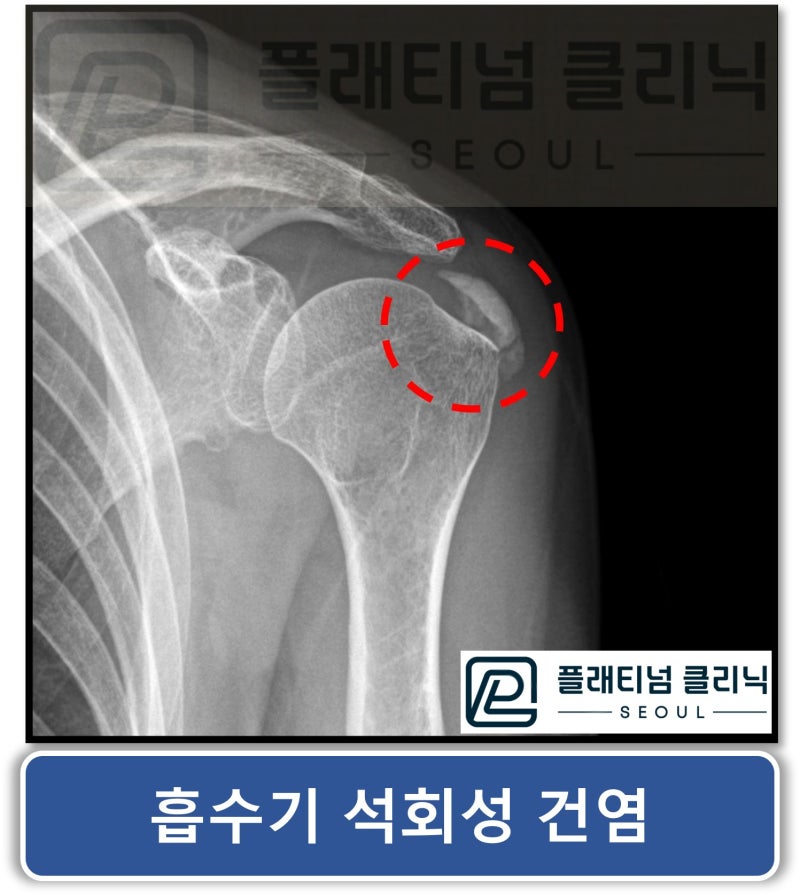
On X-ray, the white area within the red circle is the calcification.
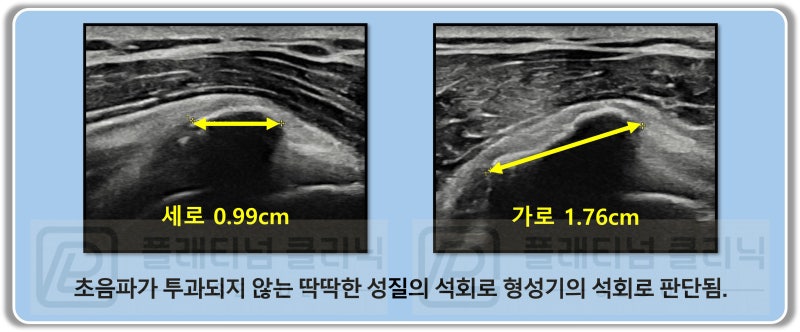
On ultrasound, because sound waves cannot penetrate solid materials, the area below a hard substance like bone appears black. In formative-stage calcification, since it is hard like bone, the area below the calcification also appears black. This patient had a hard calcification measuring 1.76 x 0.99 cm, and it was treated with calcific deposit aspiration.
As the video shows, formative-stage calcification is so hard that no matter how much you try to aspirate, it will not come out. Calcific deposit aspiration solves this problem by using the specially manufactured (patent pending) instruments to crush the calcification, making removal possible even with hard formative-stage deposits.
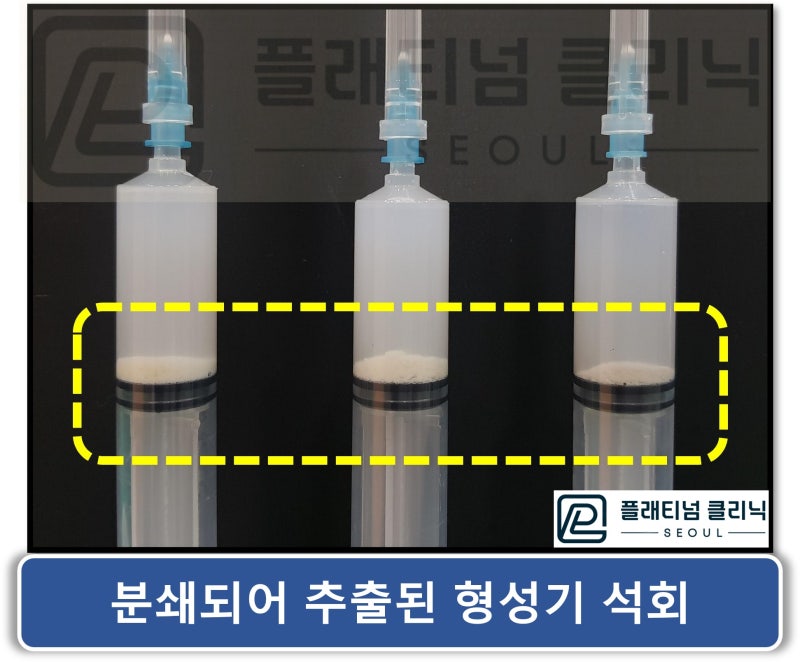
As you can see in the video, when the formative-stage calcification is crushed, it comes out like chalk dust being aspirated. Once the calcification is crushed, it turns to powder and is removed via saline irrigation.
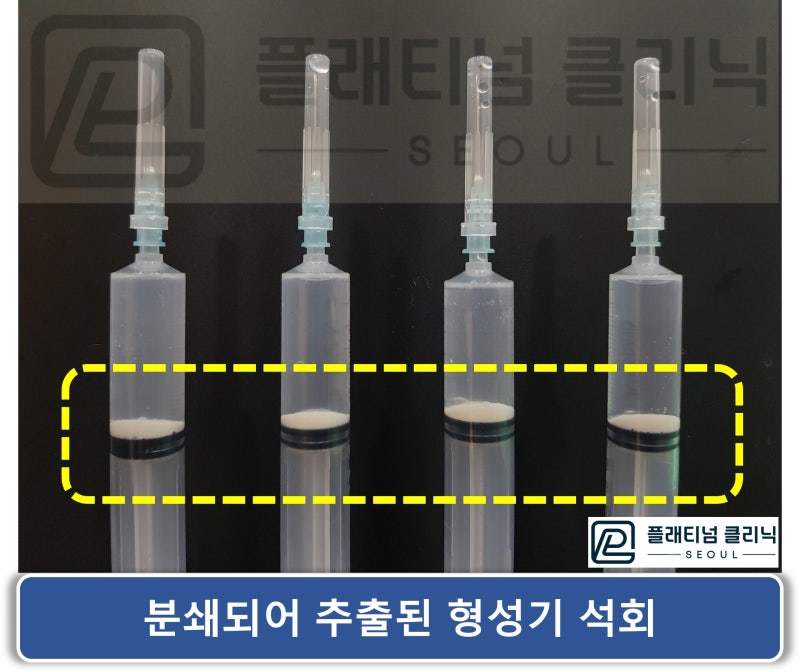
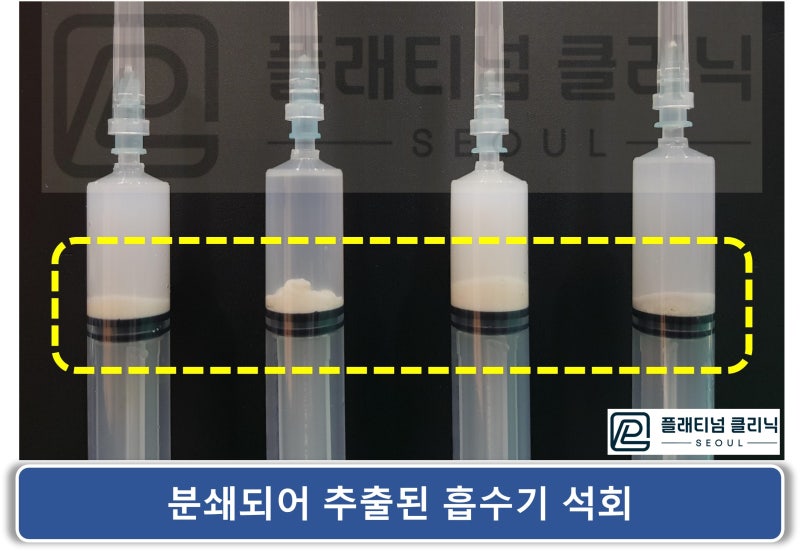
This is a photo of the syringe after calcific deposit aspiration. You can see the powdered hard formative-stage calcification has settled to the bottom of the syringe.
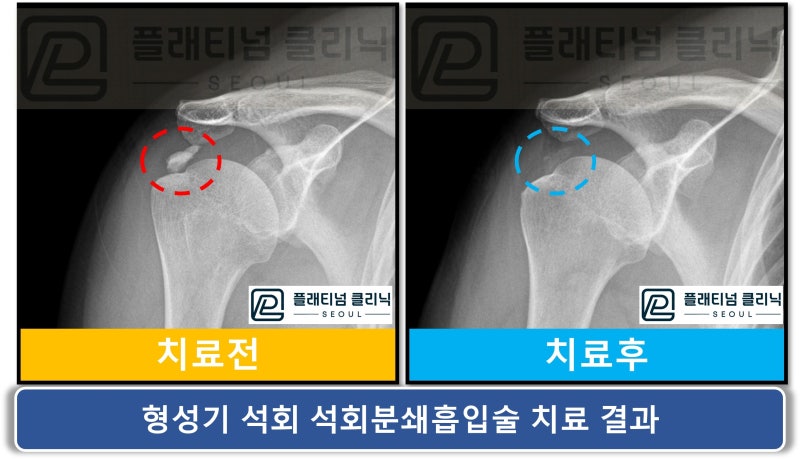
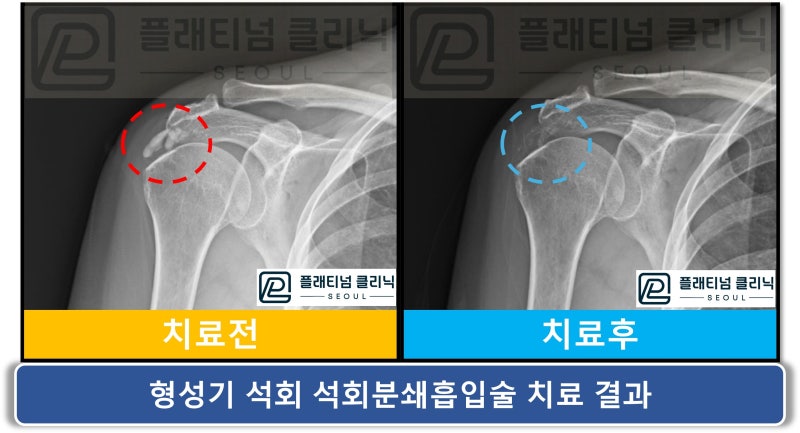
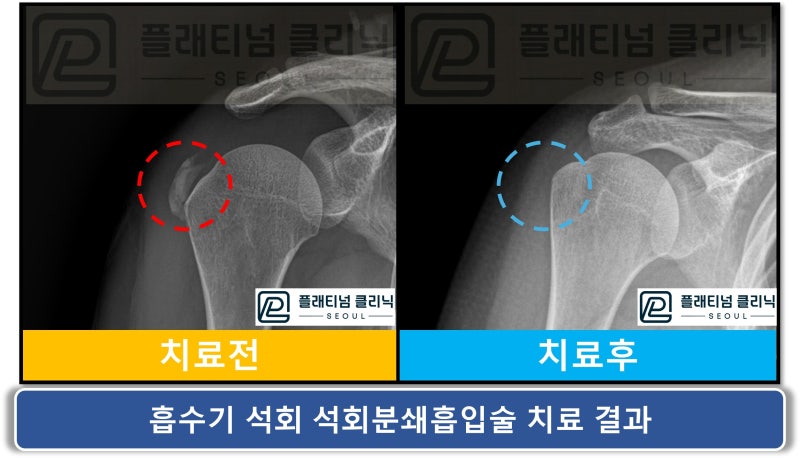
Comparing the before and after images, the calcification in the red circle has been cleanly removed and is barely visible in the blue circle. Here is another formative-stage shoulder calcific tendinitis case.

On X-ray, a large calcification is visible within the red circle. Similarly, the size and characteristics were assessed by ultrasound and determined to be a formative-stage calcification. The calcification was removed through calcific deposit aspiration.
As shown in the video, the calcification is first crushed, then a syringe filled with saline is used to remove the crushed material. You can observe the initially clear syringe gradually becoming cloudy as the calcification is aspirated.
Here is the syringe after the procedure. White powder-like calcification has settled to the bottom of the syringe.
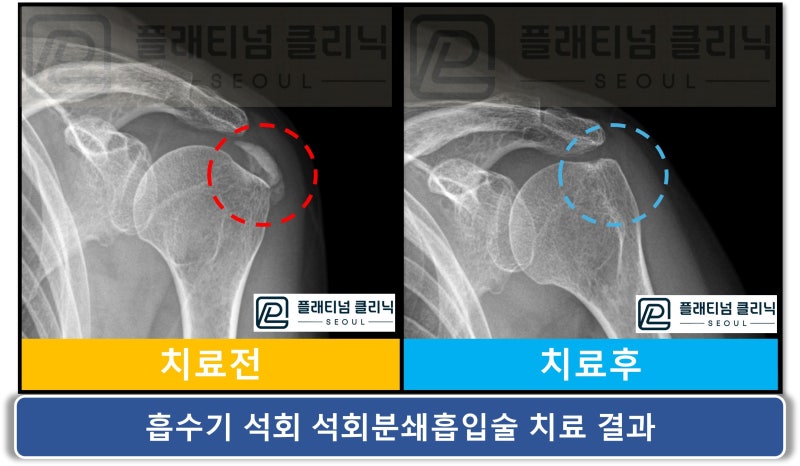
Comparing the before and after X-rays, the calcification visible in the red circle is no longer visible in the blue circle. Even with hard formative-stage shoulder calcific tendinitis, the calcification can be removed through calcific deposit aspiration. Because the calcification is so hard, removing it with a standard syringe is simply impossible. This is why many patients have been told at other hospitals: "The calcification is too hard to remove," "Let's manage with injections and shockwave therapy," or "Otherwise, you need surgery."
But I can remove even the hardest formative-stage calcifications with calcific deposit aspiration. Dr. Dongkyu Lee
Now let us look at a resting-stage calcific tendinitis case.

On X-ray, the white area within the red circle is the calcification. Based on its location, it appears to be in the infraspinatus tendon.

On ultrasound, like formative-stage calcific tendinitis, the calcification is hard so the area below it appears black. However, the calcification shape appears slightly different and extends lower compared to formative-stage calcification, which identifies it as resting-stage. Because it is also a hard calcification, simple syringe aspiration cannot remove it. Many patients tell me they had "calcification removal" done at another hospital, but the pain got worse and the calcification size did not change. When I ask what was done, they typically describe: the doctor tried to aspirate with a syringe first but nothing came out, so the area was pierced multiple times with a syringe, followed by several rounds of shockwave therapy. When they checked again, the calcification had not absorbed, so they repeated the syringe piercing and shockwave. This cycle was repeated. Symptoms did not improve, the calcification did not go away, and feeling frustrated, they came to me. Many patients come to me in this situation. Also, many patients come after going through all this treatment only to be told by the treating hospital that surgery is now necessary. Even with hard calcifications like these, with the right specialized instruments and expertise, the calcification can be removed. Calcific deposit aspiration was performed in this case as well.
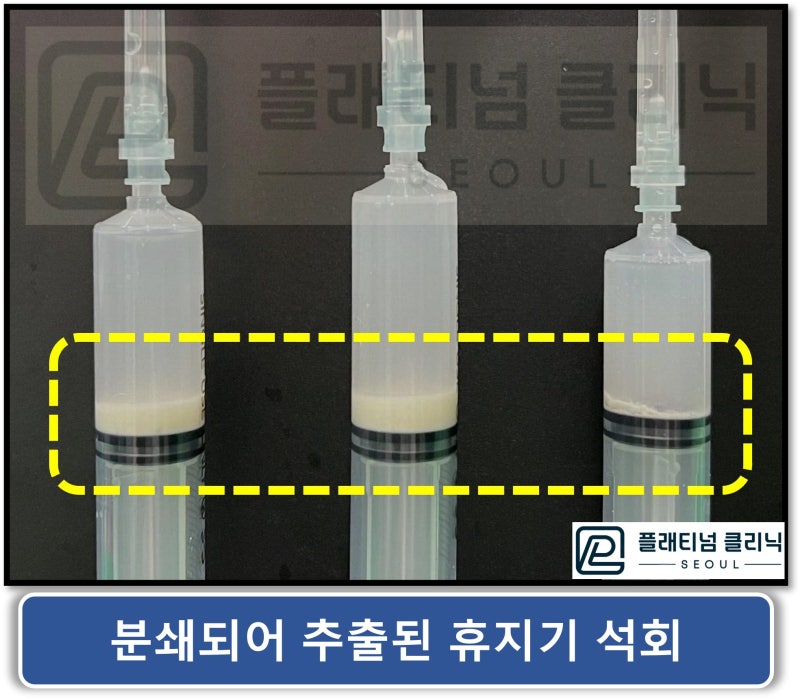
In the video above, you can see that the resting-stage calcification comes out as slightly chunky pieces rather than fine powder. It has a somewhat different appearance from formative-stage calcification.
The syringe photo after the procedure shows a large amount of aspirated calcification.
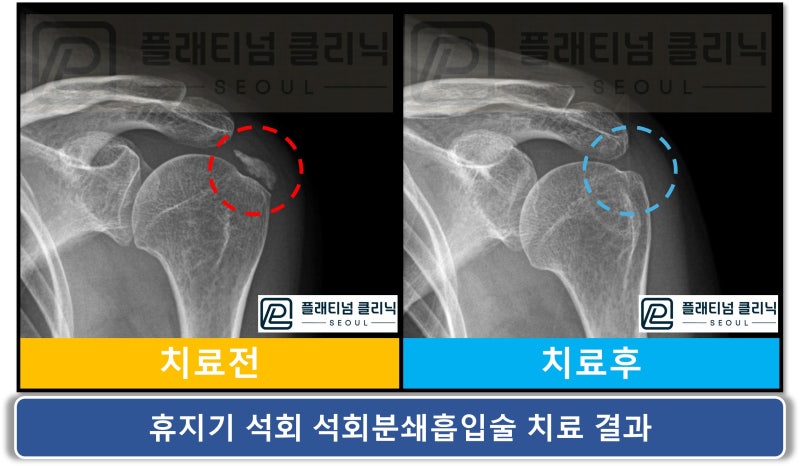
Comparing the before and after X-rays, the calcification in the red circle is no longer visible in the blue circle. The calcification has been almost completely removed. Here is another resting-stage shoulder calcific tendinitis case.

On X-ray, a large, white calcification is visible within the red circle.
In the video, the calcification comes out as slightly chunky pieces rather than powder. This is characteristic of resting-stage calcification. Even with hard calcifications like those in the formative and resting stages, my patented, specially manufactured instruments can crush and remove them.
The post-procedure syringe photo shows an enormous amount of extracted calcification.
Comparing the before and after images, the calcification has been cleanly removed. Not only hard formative-stage calcification but also hard resting-stage calcification can be removed through calcific deposit aspiration. For patients who have been told their formative or resting-stage calcification is too hard to remove, and who have only been managing pain with steroid injections and shockwave therapy, I tell them that calcific deposit aspiration can remove even these hard calcifications. I have studied, researched, and developed extensively to treat calcific tendinitis without surgery, resulting in calcific deposit aspiration and the instruments needed for it. Today, I have nearly perfected both the technique and instruments to treat patients' calcific tendinitis without surgery. Now let us look at a resorptive-stage shoulder calcific tendinitis case.

On X-ray, the calcification within the red circle looks different from formative and resting stages. It has a slightly lighter density. After seeing so many calcific tendinitis images, I can now estimate the nature of the calcification just from the X-ray. Still, to determine the exact condition, size, and location, an ultrasound examination is performed.
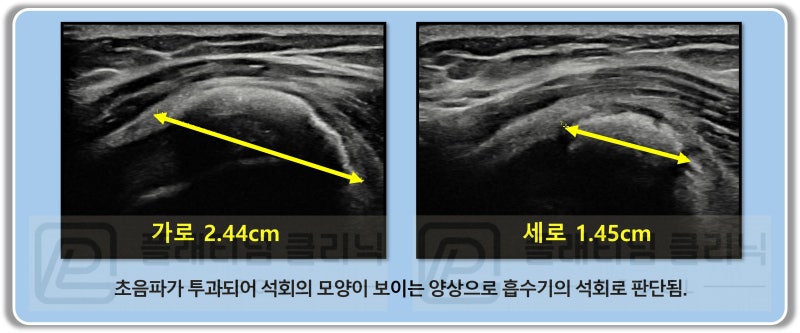
Unlike the previous ultrasound images, the full shape of the calcification is visible and appears as a bright white signal. This was a large resorptive-stage calcification measuring 2.44 x 1.45 cm. Calcific deposit aspiration was performed.
Resorptive-stage calcification has a paste-like consistency. While some can be aspirated with a syringe, the paste can sometimes clog the syringe opening, and often only some comes out while the residual calcification remains stuck. Calcific deposit aspiration addresses this by first injecting a solution that thins the paste-like calcification before aspirating. Then, any remaining calcification is crushed with the specialized instruments to remove as much as possible.
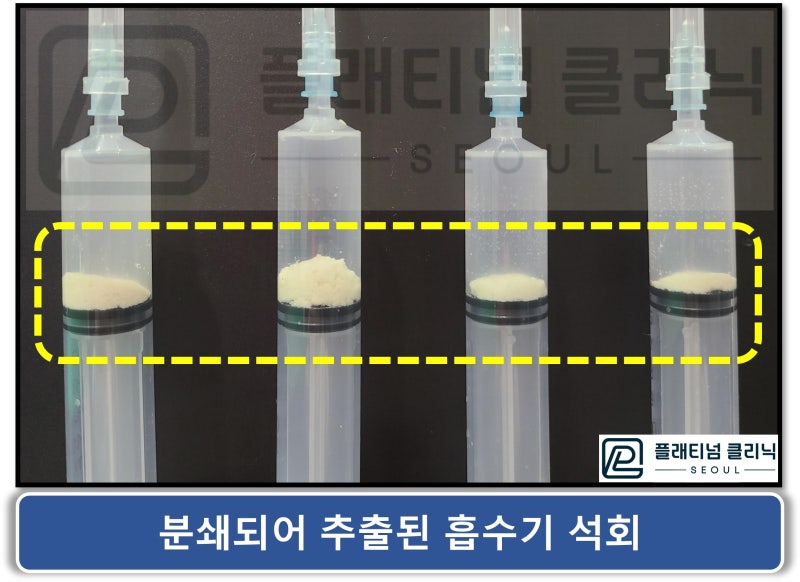
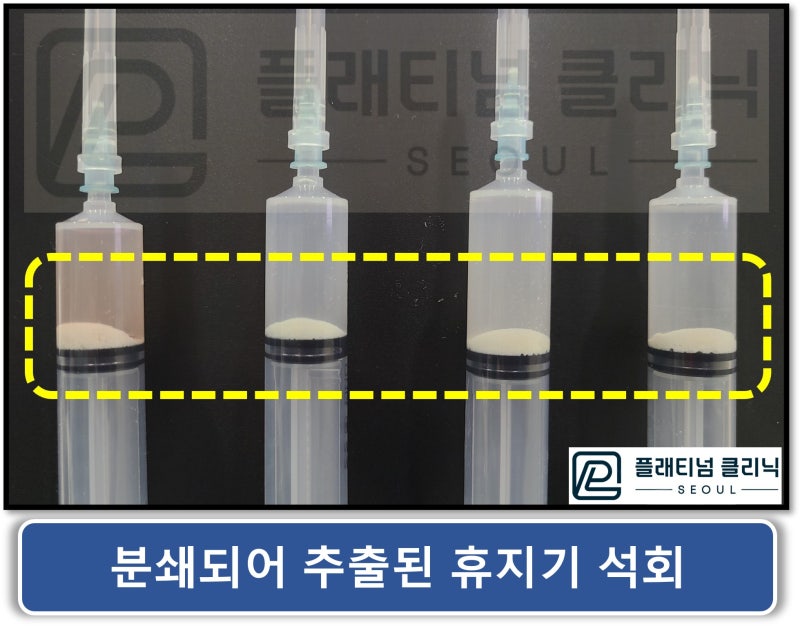
The syringe photo shows clumpy rather than powdery calcification. Because resorptive-stage calcification is paste-like, the extracted material looks different from formative and resting-stage calcification.
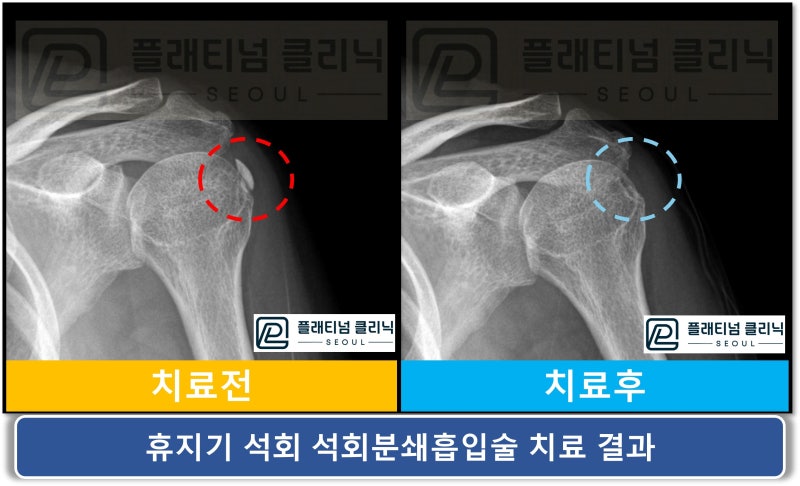
Comparing the before and after images, the resorptive-stage shoulder calcification in the red circle has been completely removed in the blue circle. Here is another resorptive-stage shoulder calcific tendinitis case.
Again, a large resorptive-stage calcification is visible within the red circle. Calcific deposit aspiration was performed.
In the video, you can see the calcification being squeezed out like toothpaste.
Resorptive-stage calcification is paste-like, so when aspirated into a syringe, it looks clumpy. The second syringe contains the initial clumpy extraction, while the rest was extracted after crushing. You can see that the amount extracted after crushing is much greater than the initial aspiration. In other words, even if you aspirate and think you have removed some calcification, the remaining amount may be much greater. Calcific deposit aspiration crushes all residual calcification and removes as much as possible.
The before and after images of the resorptive-stage shoulder calcific tendinitis treatment show complete calcification removal. Of course, there may be trace amounts of residual calcification. These may be naturally absorbed over time, and if shockwave therapy is combined after the procedure, complete removal can be achieved. I have shown you cases of calcific deposit aspiration across all stages of shoulder calcific tendinitis. I only showed 2 cases per stage, but I have experienced far more. (I believe I have performed over 10,000 cases to date.) There was one unfortunate case where a patient had undergone surgery for calcific tendinitis, but continued to have pain afterward. The pain progressively worsened over 3 months, and the patient came to see me. Examination revealed that calcification still remained, and the surgical hospital said it had "recurred." Hmm... But the bigger problem was that the rotator cuff where the calcification had been removed was now torn. Surgical treatment of calcification requires a procedure similar to rotator cuff repair, and a shaver device is used to grind away the calcification, which inevitably damages the tendon. If the calcification is large, the tendon damage is even greater, and if the tendon is weakened or does not heal properly, it can lead to tendon tears. If calcific deposit aspiration had been done from the beginning, this complication could have been avoided. But since the tear had already progressed significantly, I recommended surgical treatment. I do not believe calcific tendinitis is a condition that requires surgery. The reason is that calcification can be removed without surgery. Surgery inevitably causes tendon damage and can lead to additional complications.
Shoulder calcific tendinitis at any stage can be treated with calcific deposit aspiration. With the right specialized instruments and expertise, 99% of calcifications can be removed. Dr. Dongkyu Lee
🔗 https://platinumos.co.kr/