Re-tear After Rotator Cuff Surgery: What Went Wrong? Recently, the number of patients requiring revision surgery has been noticeably increasing. Among patients who have visited our clinic with persistent pain, lack of functional recovery, and no improvement after rotator cuff surgery months or even years ago, many unfortunately need surgery again. What is even more unfortunate is that most of these patients are relatively young. Some could have been fully healed with a single surgery if the initial diagnosis and surgery had been done properly, while others had surgery unnecessarily when it was not needed, leading to re-tears that now require revision surgery. Let me discuss one such case. The patient fell and injured the shoulder several years ago. However, the injury was neglected, and when symptoms did not improve, the patient underwent MRI at another hospital followed by surgery. The patient was told there was calcific tendinitis and had surgery to remove it and repair the ligament. Let's review the imaging from that time.
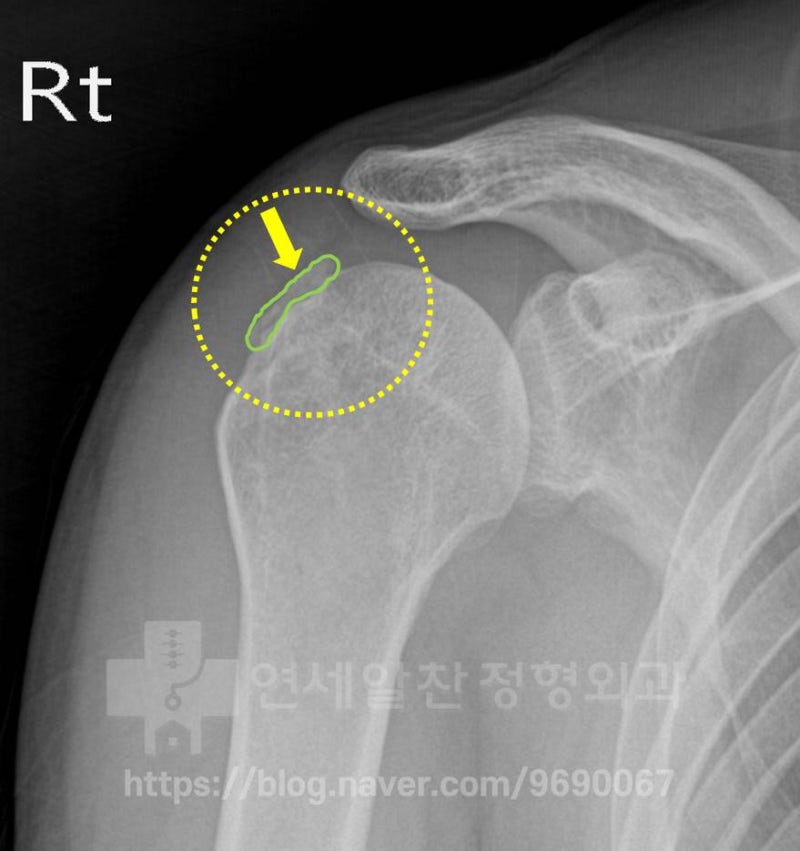
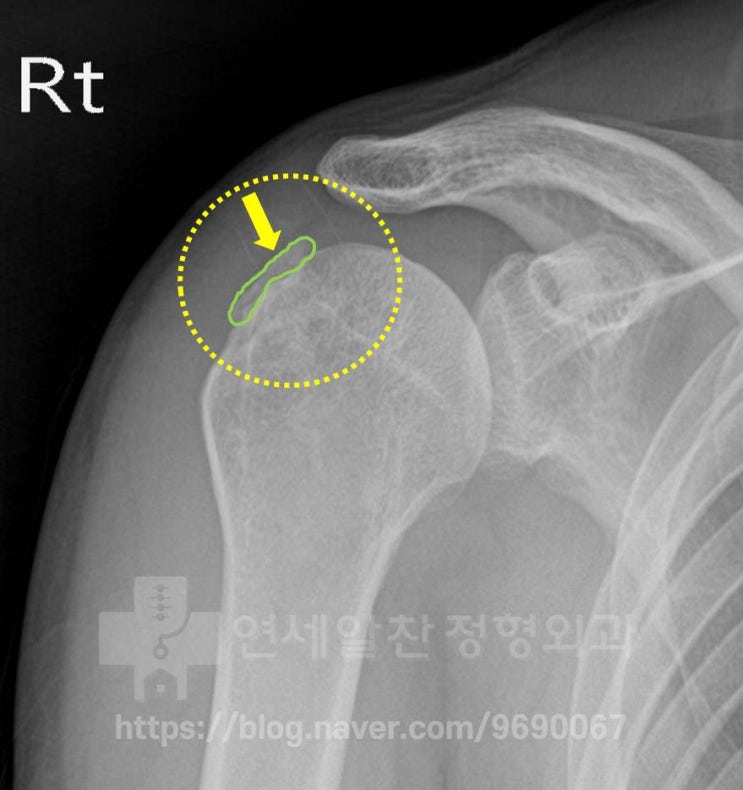
On X-ray, what appears to be calcification is visible in the area marked with the green line. Let's look at another X-ray.
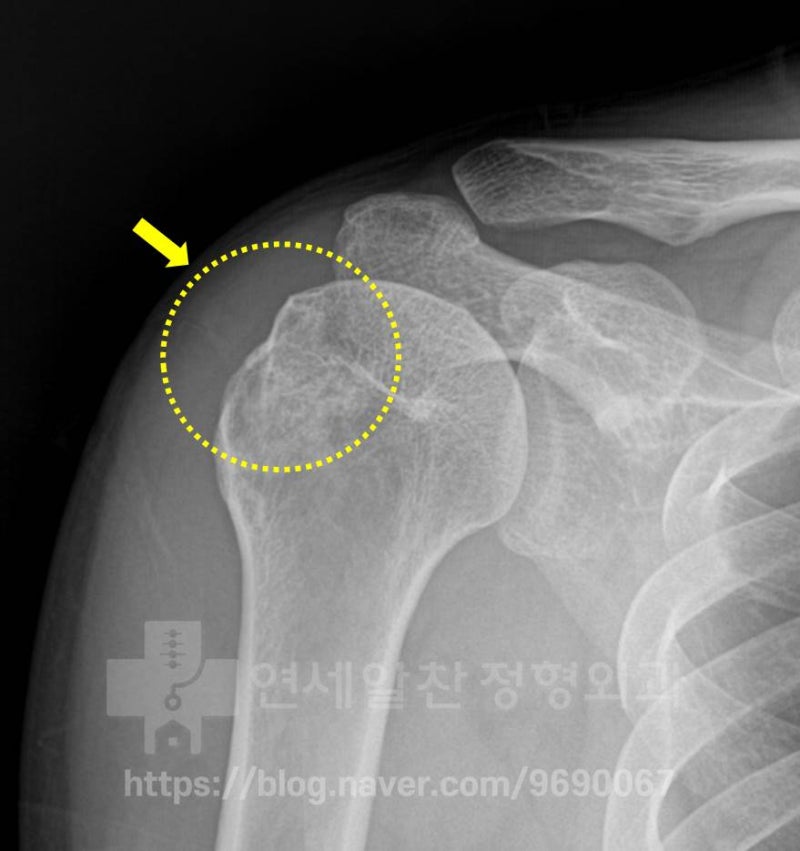
In the area marked with the yellow dotted line, the greater tuberosity of the humerus appears abnormal, as if something was damaged.
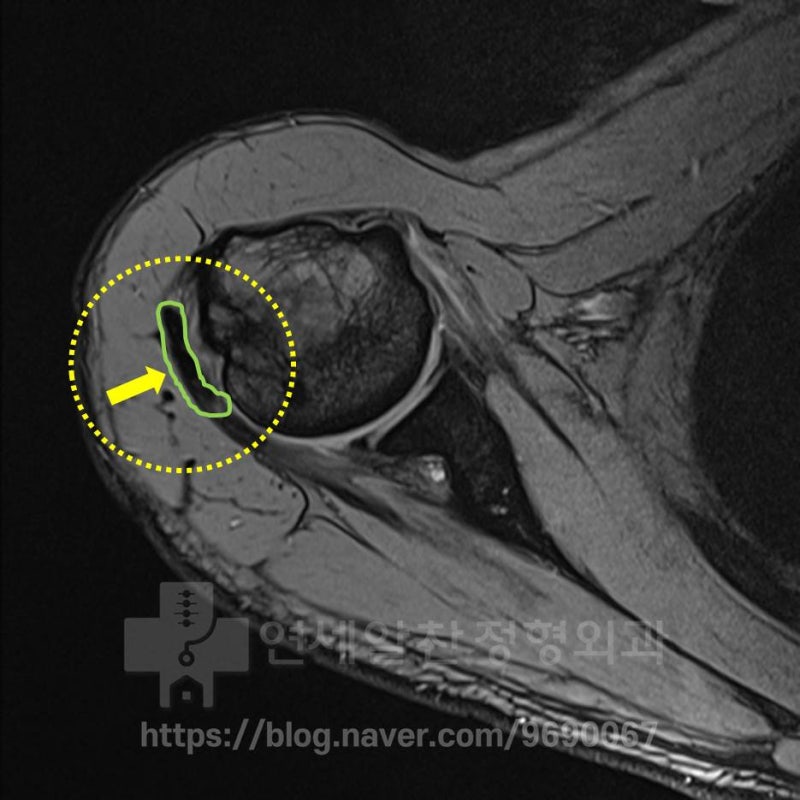
On MRI, a dark shadow is visible in the area marked in green.
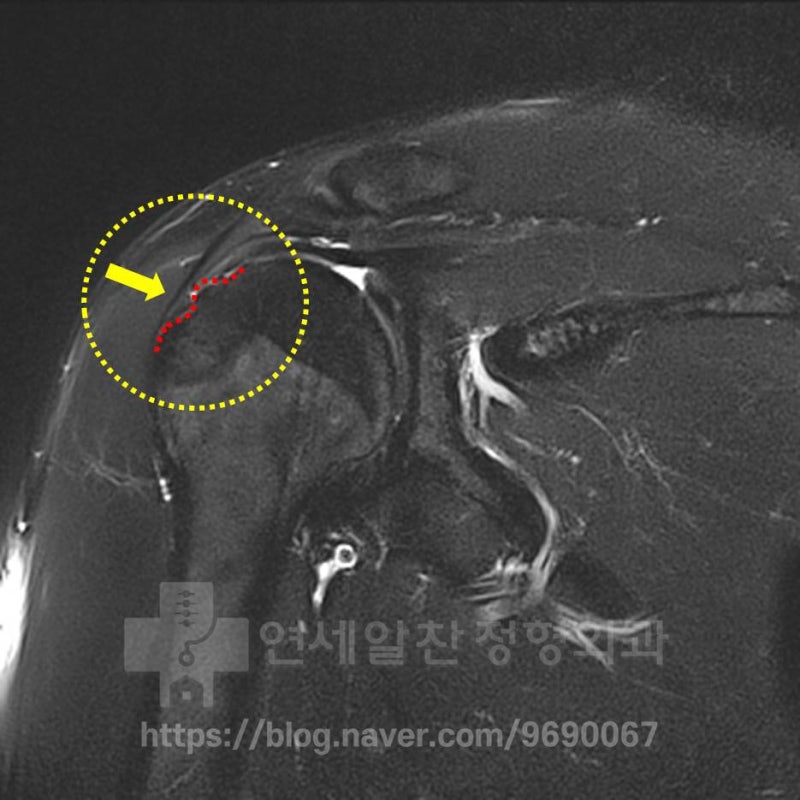
On another MRI, an irregular surface of the greater tuberosity is observed in the area marked with the red dotted line. However, while supraspinatus weakening is observed, no tear is visible. Considering the patient's mechanism of injury and the above findings, this appears to be a case of greater tuberosity fracture nonunion rather than calcific tendinitis. The most unfortunate thing is that if proper treatment had been provided immediately after the initial injury (given the extent of damage, surgical treatment for the greater tuberosity fracture), the patient would be living and exercising normally by now. Let's review the surgical footage from that time.
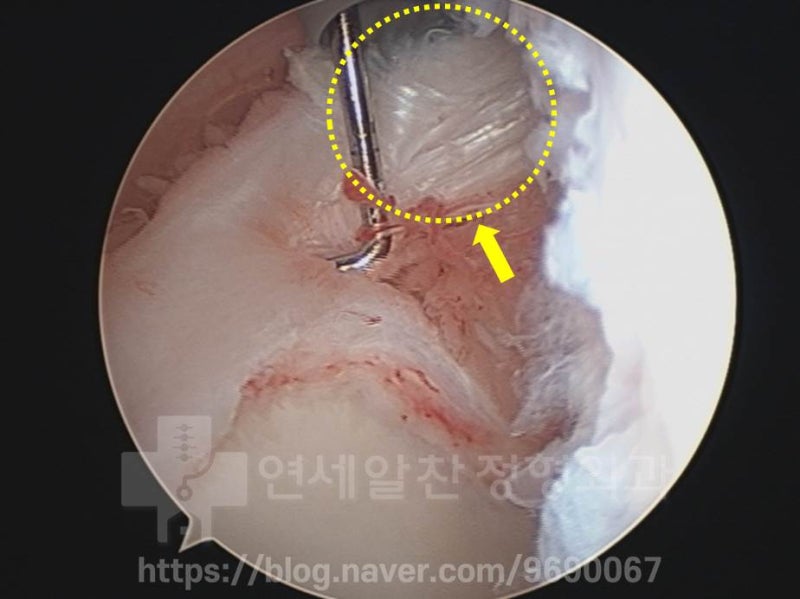
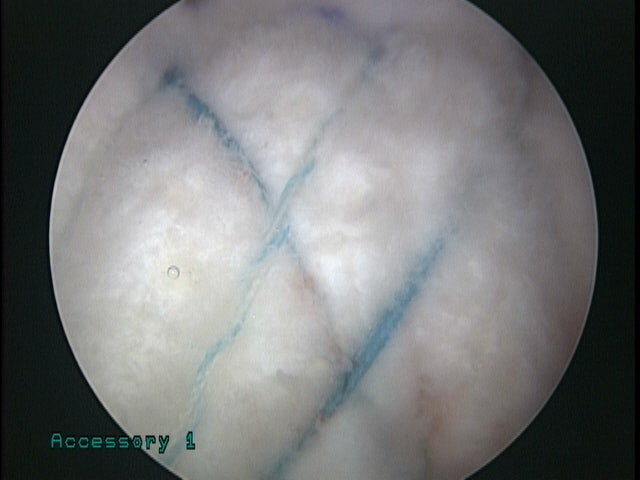
On the arthroscopic image, the area marked with the yellow dotted line shows the long head of the biceps tendon with a partial tear.

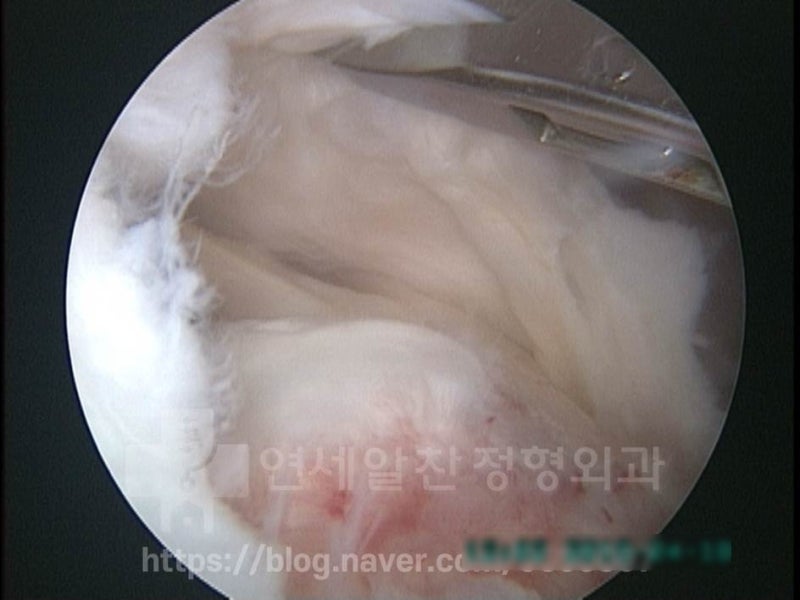
The area marked with the red dotted line appears to be a bone fragment, and the supraspinatus tendon has been almost completely dissected to remove it.

A considerably large bone fragment was removed.

After removing the bone fragment, the supraspinatus was repaired. Let me point out the issues: 1. Since there was a partial tear of the biceps tendon, it should have been either excised or fixed during the rotator cuff surgery. 2. With more careful diagnosis, it would have been identified as greater tuberosity nonunion rather than calcific tendinitis. Surgery for nonunion would have yielded much better results, considering that the supraspinatus was not torn and the bone fragment was large. Fragment fixation and ligament reinforcement would have been the appropriate surgery for this patient. Unfortunately, on the MRI taken the day after surgery, displacement of the suture anchor was observed, strongly suggesting the ligament was not properly fixed... The patient continued to experience pain and weakness, unable to raise the arm, managing with injections and medications. Recently, after getting an MRI at another hospital, the patient came to our clinic. Let's examine the condition at the time of the visit.
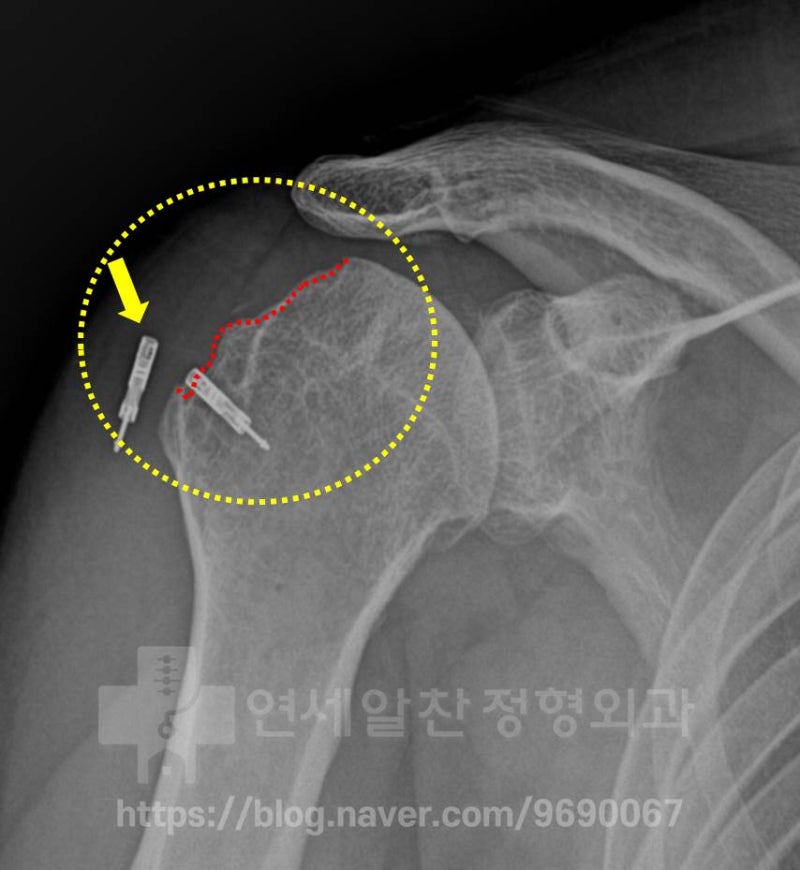
The bone loss at the greater tuberosity, marked with the red dotted line, has worsened significantly. Additionally, the suture anchor from the previous surgery (yellow arrow) has pulled out of the bone.

The MRI also shows severe bone loss at the greater tuberosity and the supraspinatus tendon is as thin as paper, severely weakened and torn. Revision surgery in this condition is very daunting. The patient is young but the ligament is in very poor condition, and the bone loss of the humerus is severe. Even with the best surgical technique, predicting outcomes comparable to the original is difficult. Given this situation, no doctor would readily volunteer for revision surgery. The patient came to me with difficulty and we decided to proceed with revision surgery.

As before, the partial tear of the biceps tendon had progressed further, so biceps tenotomy was performed. The excised biceps tendon was then used to augment the weakened supraspinatus during repair.

The yellow arrow indicates the suture anchor from the previous surgery, which had pulled out of the bone and was dangling. This was removed and the rotator cuff repair was performed.
The supraspinatus was found to be severely weakened, as thin as paper. Simple repair alone would not provide adequate tendon strength, so a hybrid suture technique was used for double-row repair, with additional augmentation using the biceps tendon and artificial ligament (MegaDerm).
Very secure repair was confirmed. After sufficient time had passed following surgery, MRI was performed again to check the status.

The supraspinatus tension appears excellent, and the dark area (yellow arrow) represents the artificial ligament augmentation, which completely covers the irregular greater tuberosity and shows good integration with the original supraspinatus. Most importantly, the patient no longer experiences the pain felt before surgery and is very happy. Muscle strengthening and functional recovery will continue to improve gradually through dedicated rehabilitation. What this case teaches us is that when the initial specialist's diagnosis is wrong, it leads to poor treatment outcomes for the patient. As with this patient, an incorrect diagnosis leading to unnecessary surgery means the patient never receives proper treatment, misses the treatment window, and the condition worsens even while visiting hospitals.
