A 54-year-old female patient came to Platinum Clinic limping on her right leg. She presented with sudden onset of pain starting 3 days prior, difficulty bending the knee, and difficulty walking. Physical examination showed a positive Apley External Rotation test, suggesting medial meniscus injury. X-ray and MRI examinations were performed.
X-ray showed no significant findings, and the scanogram revealed a well-maintained mechanical axis.
As indicated by the arrow, a tear of the medial meniscus posterior horn root was observed.
As indicated by the arrow, a tear of the medial meniscus posterior horn root was observed.
As indicated by the arrow, a tear of the medial meniscus posterior horn root was observed.
Damage to the medial femoral cartilage was observed.
When the posterior horn root of the meniscus is torn, the function of that meniscus is lost, leading to secondary cartilage damage that can rapidly progress to osteoarthritis. Additionally, damage to the medial femoral cartilage was already present. Surgical repair of the meniscus posterior horn root tear and chondroplasty were planned.
As shown in the surgical diagram, the plan was to repair the medial meniscus posterior horn root using an endo-button.
A complete tear of the medial meniscus posterior horn root was observed.
This is the appearance after the torn area was debrided and cleaned using a shaver.
After decorticating the root attachment site using a curette, sutures were placed.
A tunnel was created through the tibia using an ACL guide to allow passage of the sutures, which were then secured with an endo-button.
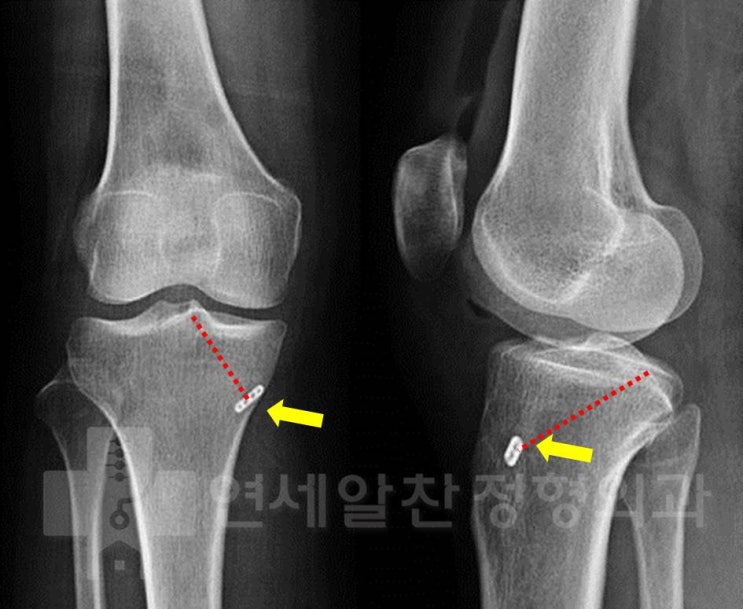
Postoperative X-ray confirms that the tunnel was accurately created in the correct position.
As indicated by the arrow, the cartilage that should normally appear white and smooth was confirmed to be damaged.
For proper cartilage regeneration, the damaged cartilage must be removed down to the subcortex.
A total of 6 microfracture holes were created.
After releasing the tourniquet, bone marrow was confirmed to be flowing well from each hole.
When the meniscus is torn, restoring its lost function is essential to prevent secondary arthritis development. Suture repair of a meniscus posterior horn root tear requires great precision and is technically challenging due to spatial constraints. However, performing this surgery accurately is both our principle and our duty.
