
Hello, I'm Dr. Dongkyu Lee, an orthopedic specialist. Shoulder calcific tendinitis... so many patients suffer from this condition. The conservative treatments for calcific tendinitis are essentially limited to injections (anti-inflammatory injections) and extracorporeal shockwave therapy. However, anti-inflammatory injections only reduce inflammation caused by calcific tendinitis to decrease pain — they don't fundamentally treat the calcium deposit itself. Extracorporeal shockwave therapy works through both mechanical stimulation and improved blood flow via cellular vibration. This helps with calcium absorption and tissue regeneration. But when the calcium deposit is large or depending on its characteristics, the treatment effect can be minimal, and in many cases the calcium is barely absorbed at all. This is why so many patients are diagnosed with calcific tendinitis and continue receiving injections and shockwave therapy, only to experience temporary improvement followed by recurring pain. Many end up suffering for years before ultimately resorting to surgery. At most hospitals, the only options offered are injections and shockwave therapy. If those don't work and symptoms persist, surgery is typically recommended. So is there truly no other treatment for calcific tendinitis? Absolutely not. There is a non-surgical procedure called calcific deposit crushing and aspiration. Calcific deposit crushing and aspiration involves crushing the calcium internally, then aspirating the crushed fragments — all non-surgically. Patients often come to me saying they had a procedure at another clinic where a syringe was used to try to extract the calcium (calcific deposit aspiration), but were told:
The calcium is too hard to extract. The calcium is too thick and viscous to extract. The calcium is too large to aspirate.
And the recommendation they heard most often after that was surgery. Depending on the nature of the calcium (hard, thick and viscous, etc.), the method of crushing it differs, and depending on the size and location, the aspiration technique varies as well. Simply inserting a syringe into the deposit and trying to withdraw it rarely works — with very few exceptions, it's ineffective in most cases. Calcific deposit crushing and aspiration can crush and remove calcium regardless of its consistency or size, making it a non-surgical procedure that can fundamentally treat most cases of calcific tendinitis. The case I'd like to share today involves a patient who had been suffering from calcific tendinitis for years. Like many others, she had been continuously receiving injections and shockwave therapy, experiencing repeated episodes of pain. Shortly before visiting me, her pain had become extremely severe. She received a calcific deposit aspiration at her previous clinic, but was told the calcium was too large and too thick to extract — and was advised to have surgery. Let's take a look at the case.

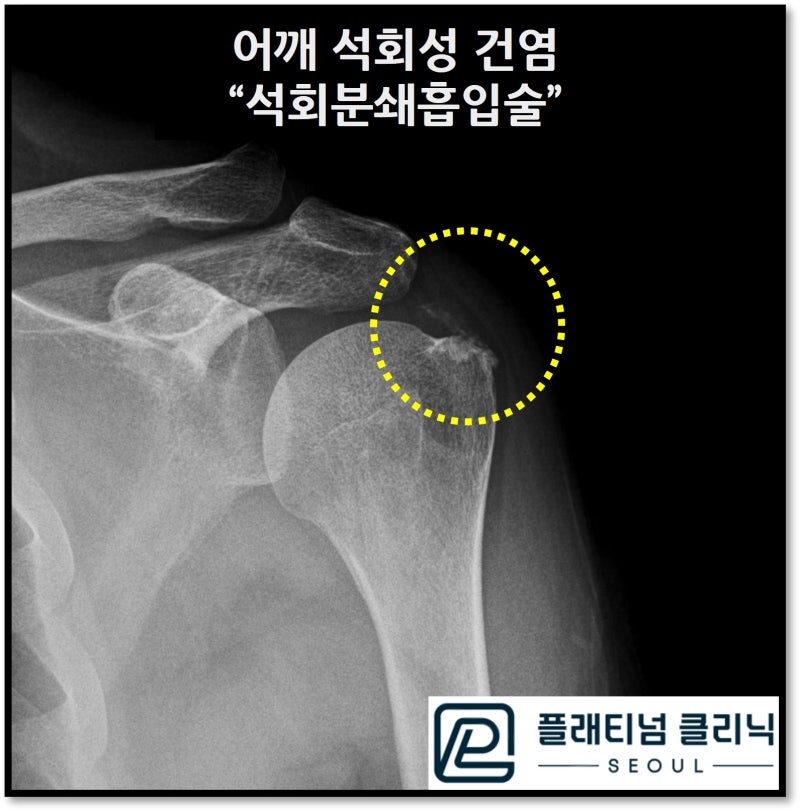
On the X-ray, an enormous calcium deposit is visible within the red circle. Ultrasound measurement showed it was 2.7 x 2.0 cm — large enough to occupy almost the entire supraspinatus tendon. With a deposit this enormous, surgery carries a high risk of damaging the supraspinatus tendon, and there's a good chance not all the calcium could be removed even surgically. I performed calcific deposit crushing and aspiration. The procedure begins with pain management. A brachial plexus block is administered, followed by additional sedation. In this patient's case, with an extremely thick and enormous calcium deposit, the approach was to first soften and crush the viscous calcium internally, then aspirate it.
In the video, you can see the softened, viscous calcium emerging in massive quantities — like toothpaste being squeezed from a tube. Afterward, the remaining calcium is crushed and aspirated through several more cycles.

Looking at the post-procedure syringe, the white material settled at the bottom is the removed calcium. An enormous amount of calcium came out. Now let's see the results.
The post-procedure X-ray shows that the calcium deposit visible at the start has nearly disappeared. The vast majority of the calcium has been removed. Let's compare the before and after images once more.
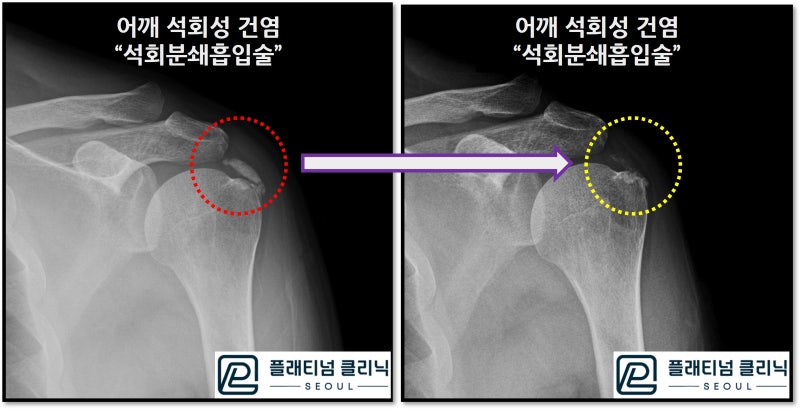
This side-by-side comparison clearly shows that the calcium has been almost completely absorbed. The entire procedure was performed through just a single guide needle, with no additional tendon damage and no wound. The procedure went very well. Of course, since the calcium had occupied nearly the entire supraspinatus, proliferation therapy was also administered to address tendon weakening and partial damage. When the patient returned to the clinic a week later, she said the pain she had been living with had simply vanished. She was thrilled to finally be free from pain and wondered why she had suffered for so many years when this treatment had been available all along.
Shoulder calcific tendinitis — don't endure the pain in silence. It can be fundamentally treated with calcific deposit crushing and aspiration.
Next time, I'll show you a case of treating hard-type calcific tendinitis.
