Some people think surgery is always the best option for a shoulder cyst. However, if there is no accompanying labral tear, cyst removal surgery is not always necessary. So what exactly is a labral tear, and when is cyst removal surgery appropriate?
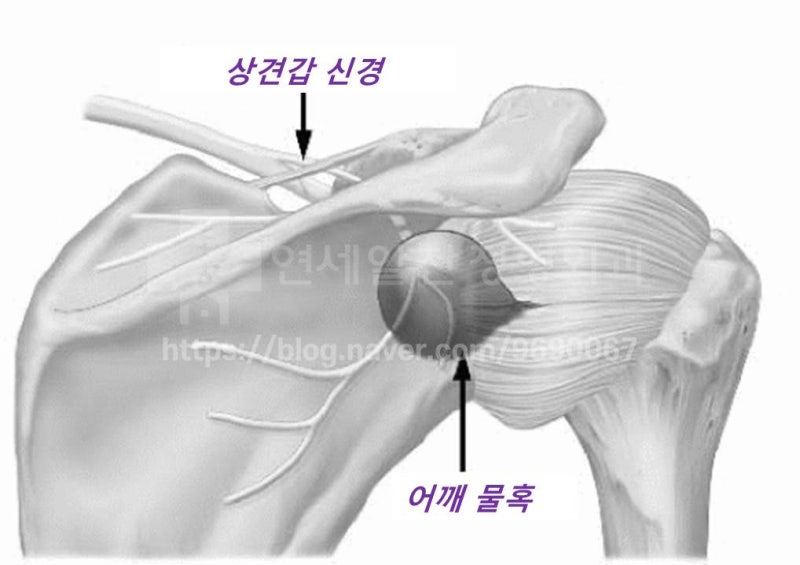
First, a shoulder cyst refers to a spinoglenoid cyst that develops where the suprascapular nerve passes through the scapula. As shown in the diagram, when a cyst develops where the suprascapular nerve travels, it can cause atrophy and weakness of the supraspinatus and infraspinatus muscles that this nerve innervates, along with numbness and pain radiating to the posterior shoulder and upper arm. So how do these shoulder cysts develop? While they can occur without a clear cause, most cases arise from joint fluid leaking out due to labral tears. Most commonly, superior labral tears (SLAP lesions) are frequently associated with spinoglenoid cysts. So how should shoulder cysts be treated? For simple cysts, the treatment only needs to relieve the nerve compression by removing the cyst. Cyst removal surgery is not necessary in these cases; aspiration with a needle is sufficient. But what about cases with an accompanying labral tear or SLAP lesion? When the labral tear or SLAP lesion has not healed, surgical treatment is needed to remove the cyst and repair the labrum. Even if the cyst is aspirated, it is likely to recur if the labrum has not healed. However, if the labral damage is minimal or has already healed, aspirating the cyst with a needle followed by appropriate treatment can yield excellent results. This requires careful MRI evaluation and accurate physical examination. So performing cyst removal surgery on every case is not advisable. Let's look at a patient case. The patient developed pain after weight training and had been experiencing shoulder pain, surrounding numbness, and muscle weakness for about a year. The patient had received multiple steroid injections at other hospitals, but symptoms only improved briefly before progressively worsening. The patient was then told surgery was needed and came to our clinic for a second opinion. Let's examine the MRI taken at the other hospital.
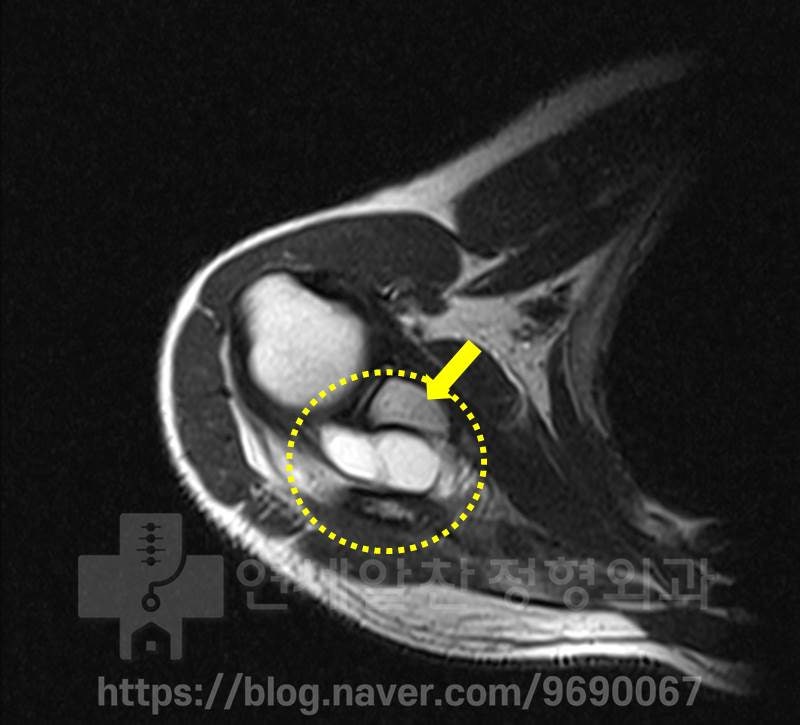
The white area within the yellow circle is the shoulder cyst. A very large cyst is visible. However, no labral damage was observed.
Again at a similar location, a large shoulder cyst is visible, with no labral damage confirmed.
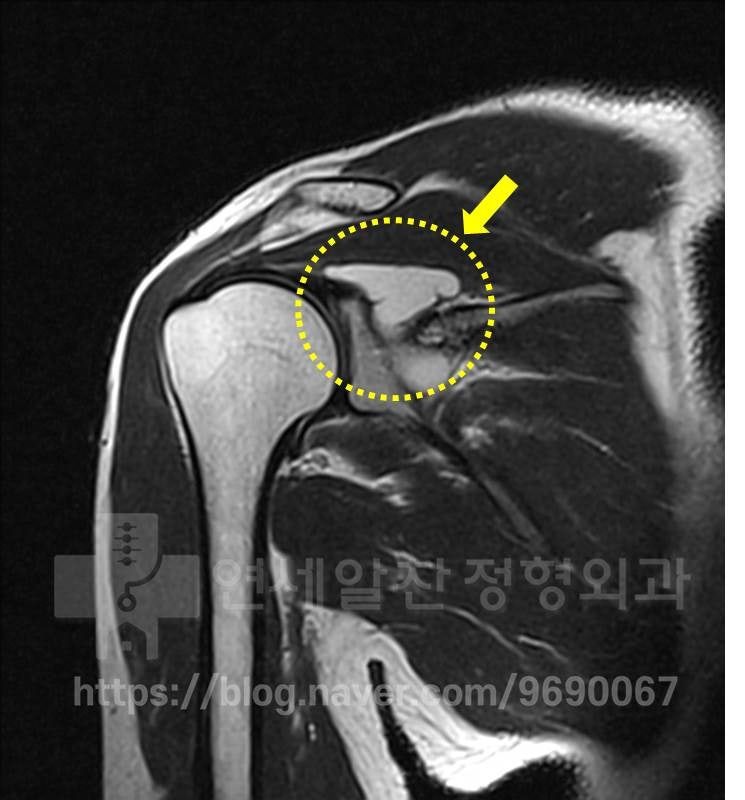
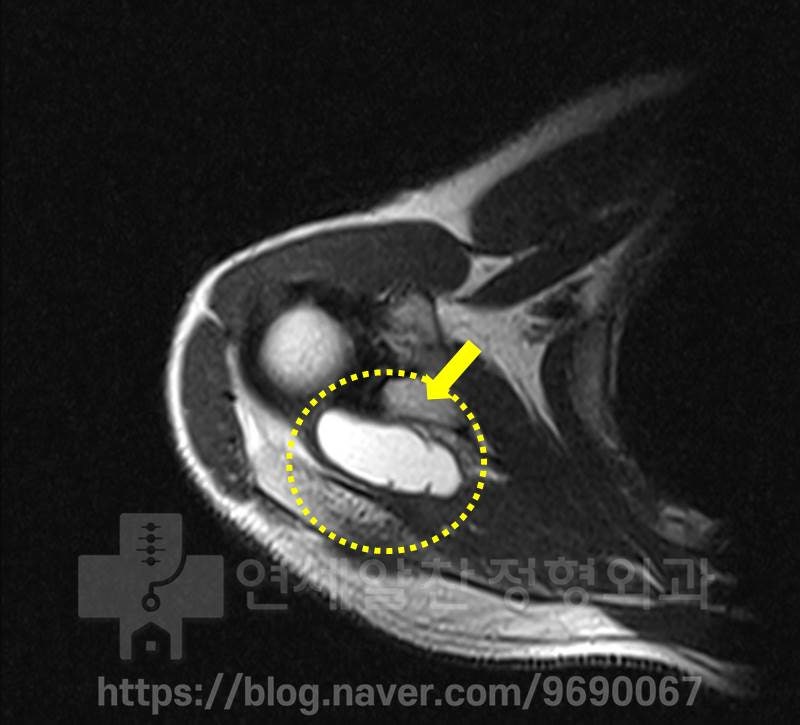
On another MRI angle, a large shoulder cyst is also visible. No superior labral damage is identified in this area.
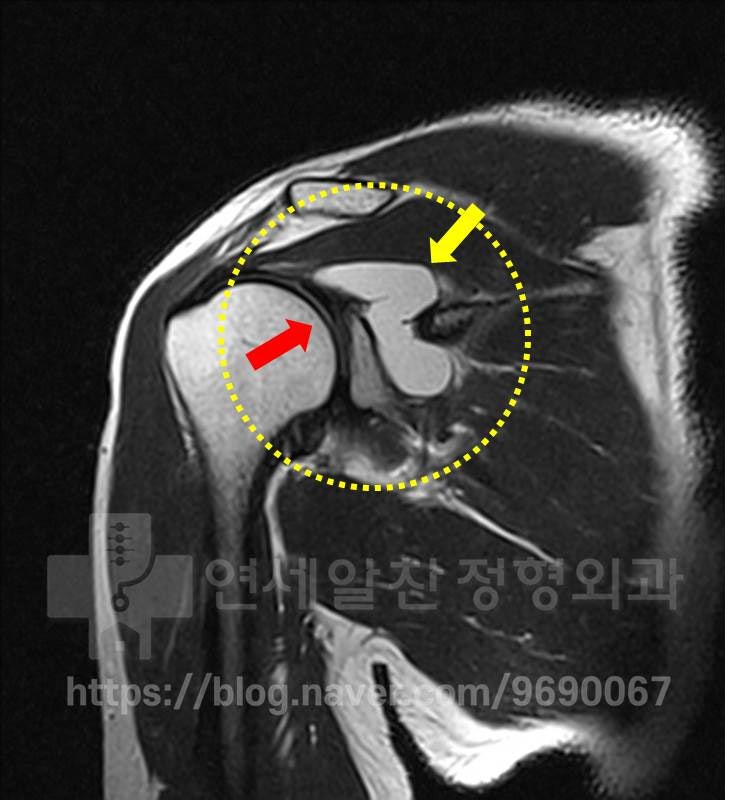
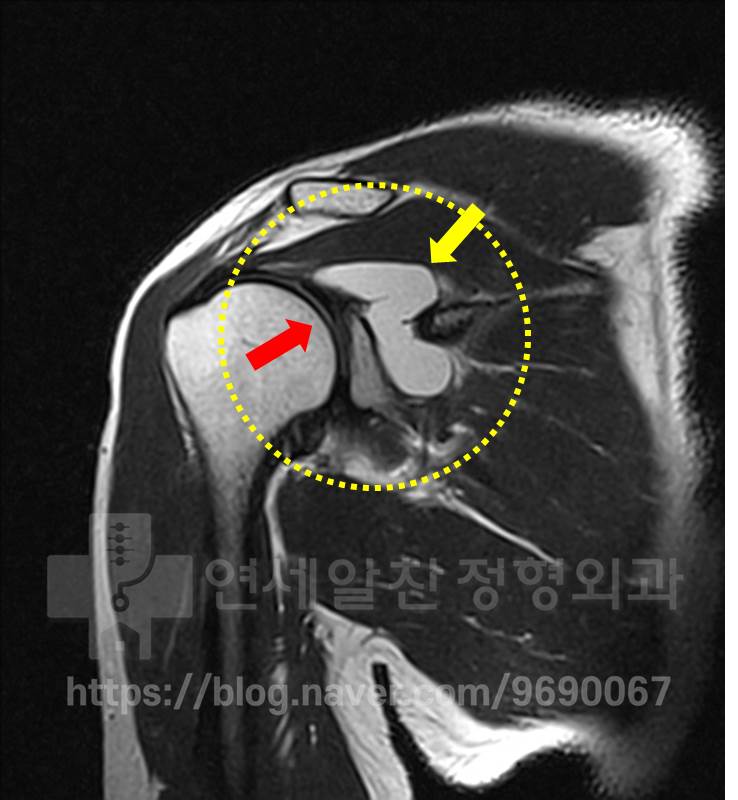
The shoulder cyst is again visible on MRI. A slight trace of superior labral damage is observed in the area marked in red, but it appears to have already healed. Physical examination showed no findings suggestive of a SLAP lesion, while tests for supraspinatus and infraspinatus weakness were positive. In this patient's case, the labral damage was minimal and appeared nearly healed, with symptoms attributable to the large shoulder cyst. Therefore, we decided to remove the cyst via ultrasound-guided needle aspiration.
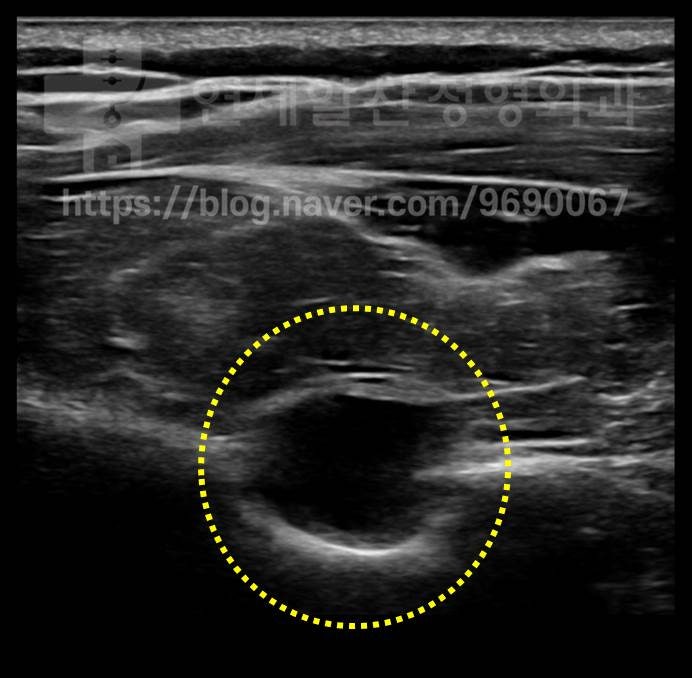
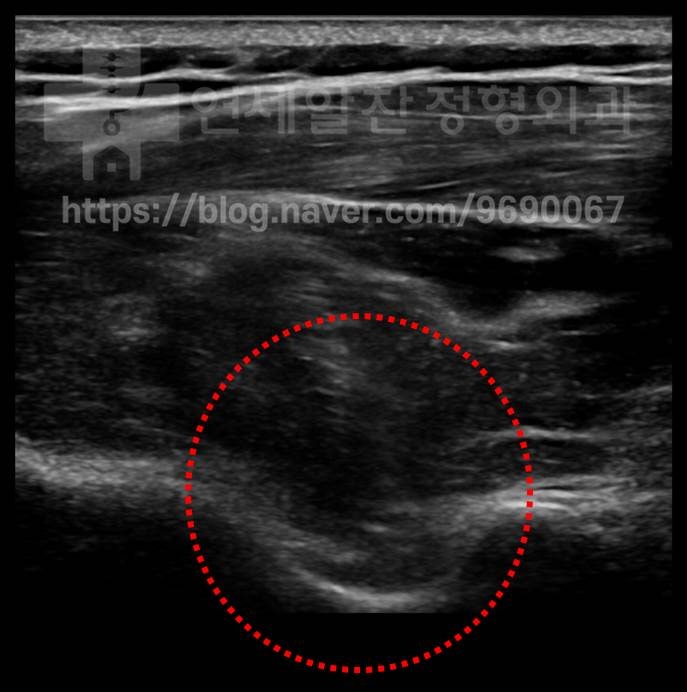
On ultrasound, the dark area within the yellow circle is the cyst.
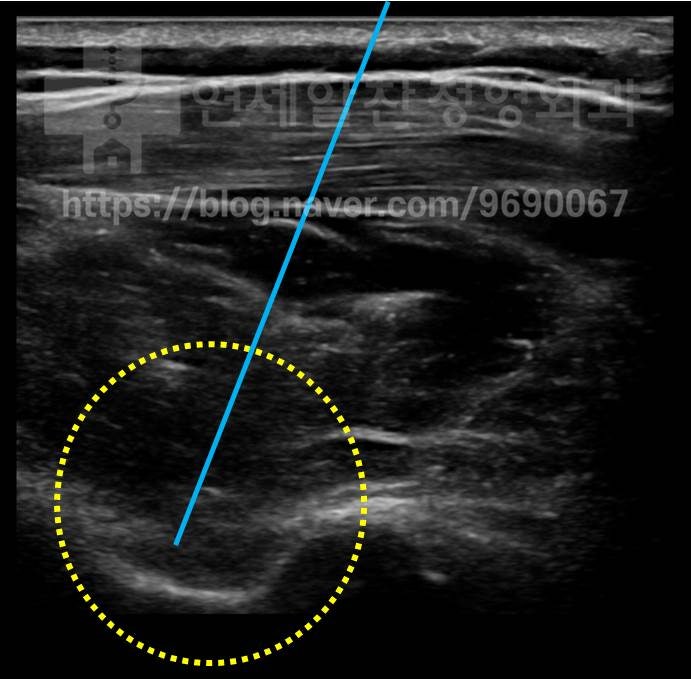
After confirming the location with ultrasound, a needle (blue line) was used to aspirate the cyst. The previously visible cyst has been completely removed.

This photo shows the cyst fluid aspirated from the shoulder. Afterward, the patient's symptoms improved significantly, and muscle strength recovered considerably through progressive rehabilitation exercises. An ultrasound examination was repeated one year later.
On ultrasound, no shoulder cyst was observed, and the patient continued to enjoy sports without symptom recurrence. As demonstrated, while surgical treatment is necessary when the labrum is damaged, cyst removal surgery is not always required when a shoulder cyst is present. When labral damage is minor or has healed, non-surgical treatment such as needle aspiration alone can yield excellent results for shoulder cysts. (However, thorough physical examination and accurate MRI interpretation are essential.)
