A 47-year-old male patient presented with shoulder pain lasting more than 6 months. Despite several months of injection and medication treatment, his symptoms had not improved, and he visited Platinum Clinic for an accurate diagnosis and proper treatment. Physical examination revealed positive findings for empty can test, drop arm sign, impingement sign, speed test, and biceps load test. Damage (tear) to the supraspinatus and long head of biceps was suspected, and X-ray and ultrasound examinations were performed.
A hook-type acromion was observed, as indicated by the purple line.
Ultrasound revealed an anterior and massive tear of the supraspinatus. Due to signs of retraction on ultrasound, an MRI was performed to determine the exact surgical status. The complete tear of the supraspinatus is visible as indicated by the red arrows. There appeared to be some damage at the origin of the long head of biceps, though it was not definitive.
Given the prolonged pain and the clearly confirmed full-thickness tear of the supraspinatus, supraspinatus repair and acromioplasty were planned. The treatment plan for the biceps tendon would be determined based on arthroscopic findings.
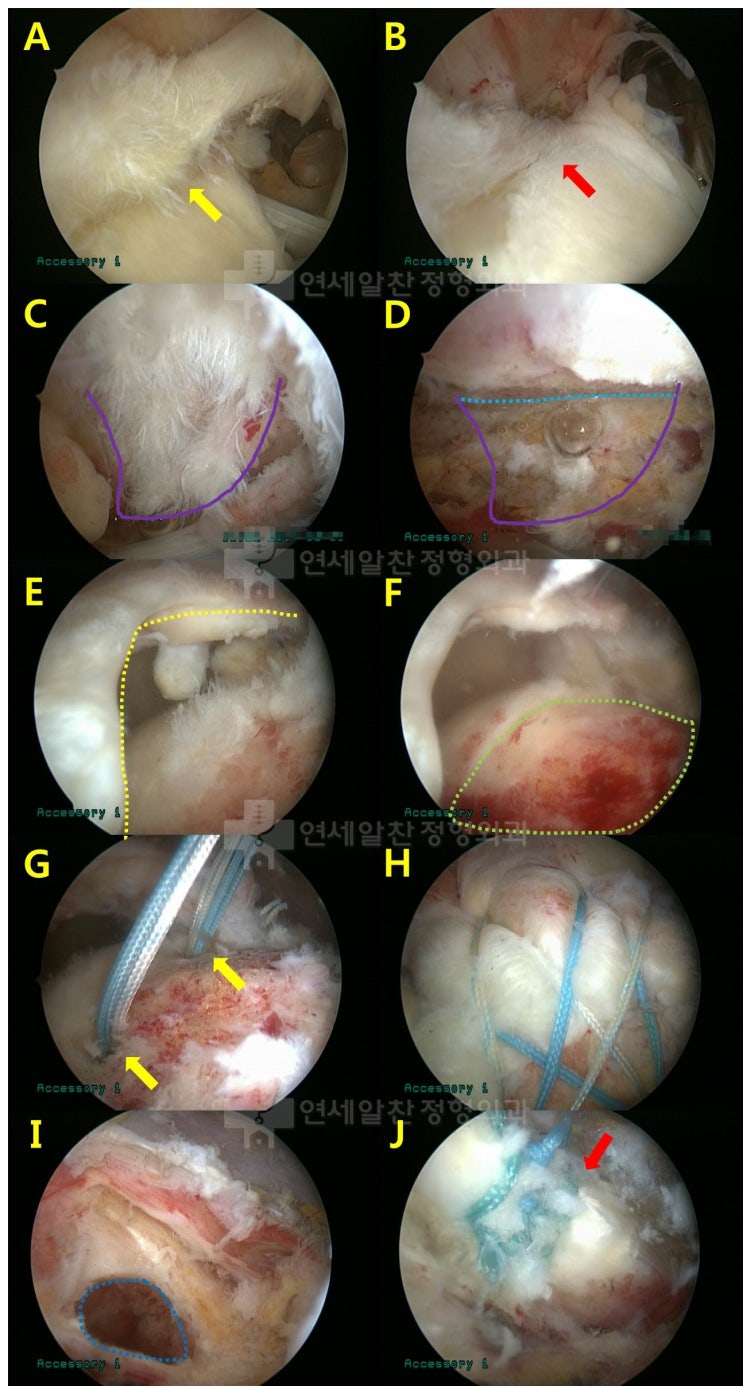
A. A partial tear was observed at the origin of the long head of biceps. Since the patient was an active worker, biceps tenodesis was decided upon. B. Tenotomy of the long head of biceps was performed in preparation for tenodesis. C. Fraying of the coracoacromial ligament was observed, and acromioplasty was planned. D. Acromioplasty was performed successfully. E. A massive tear of the supraspinatus was observed. F. Appropriate decortication of the footprint was performed to promote healing with adequate bleeding. G. Two suture anchors were inserted at the appropriate positions. H. Double-row repair was performed using the suture bridge technique, achieving a very secure fixation. I. A hole was created at the appropriate position on the humerus for suprapectoral biceps tenodesis. J. Biceps tenodesis was successfully completed.
Post-operative X-ray confirmed successful acromioplasty.
With growing interest in sports rehabilitation, various methods and theories on rehabilitation and exercise are emerging. Therapists and trainers around us are also diligently studying and advancing in these areas. What could further strengthen this effort is understanding how treatment is carried out before rehabilitation and exercise begin. I believe this knowledge leads to greater professional growth. At our rehabilitation center at Platinum Clinic, we also believe this understanding is essential. That is why we have our team observe surgeries and provide explanations about the procedures afterward, which I believe is very beneficial. Treatment and surgery belong to the physician; rehabilitation and exercise belong to the therapist and trainer. It is natural for each professional to work within their area of expertise. However, if neither understands what the other does, they end up in their own isolated league. I believe communication between these professionals is the core of sports rehabilitation.
