Many patients with adhesive capsulitis delay frozen shoulder treatment because the initial pain and movement restriction are not severe. However, as the condition progresses, pain intensifies and range of motion continues to decrease, causing severe disruption to daily life and eventually driving patients to the hospital. So when and how should frozen shoulder be treated? First, it is important to find the cause and receive an accurate diagnosis. Frozen shoulder, or adhesive capsulitis, can occur primarily without any specific cause due to degenerative changes. It can also occur secondarily due to other shoulder conditions such as rotator cuff disorders, calcific tendinitis, or labral lesions. Addressing the underlying cause of each condition is key to improving frozen shoulder treatment effectiveness. Today, let's look at a patient who received several months of treatment at another hospital without improvement. This patient had been experiencing pain and limited movement for 7-8 months before visiting us. The patient was diagnosed with frozen shoulder at another hospital and received multiple injections. However, the pain only improved briefly after each injection before returning, and the range of motion continued to worsen. We thoroughly examined the patient. The range of motion was severely limited, pain was significant, and the patient reported receiving prolotherapy injections up until one week before visiting us.
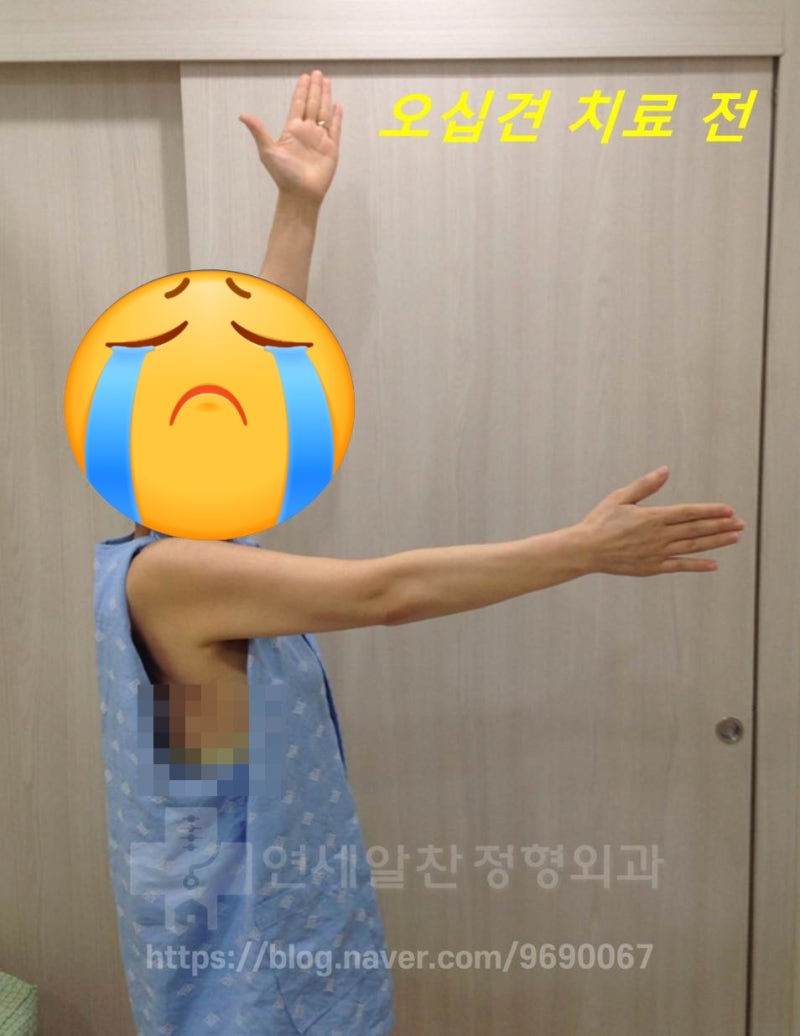
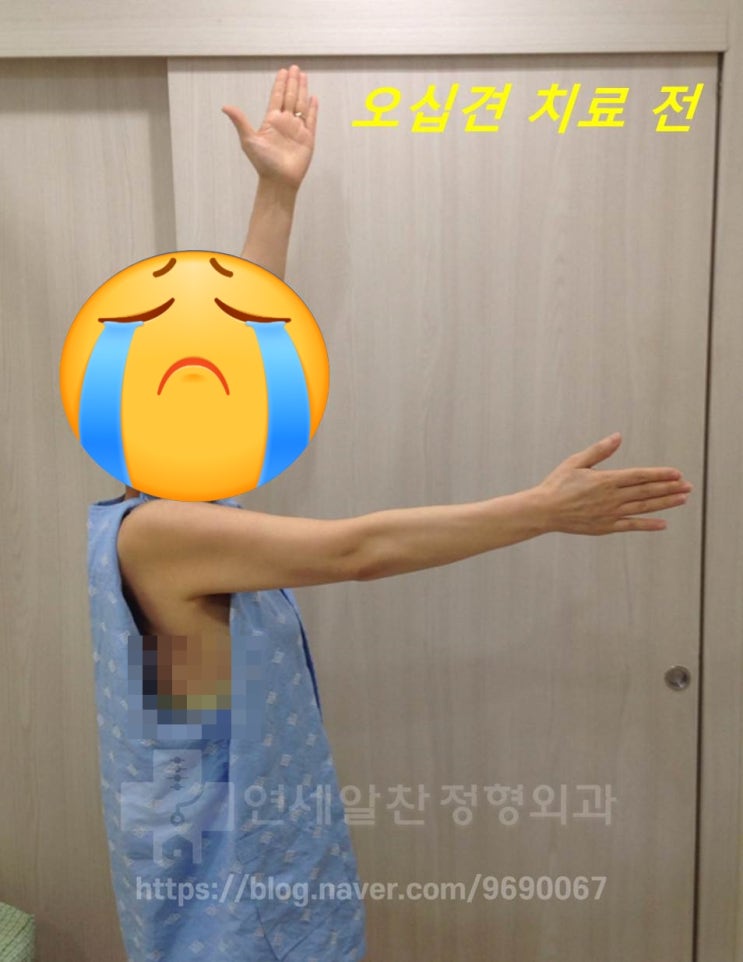
This shows the patient's range of motion checked before starting frozen shoulder treatment. Compared to the opposite side, the range of motion was significantly reduced and the scapular position was also poor. When we checked the condition through X-ray and ultrasound examination, there was no rotator cuff tear, but the joint capsule adhesion had progressed significantly. Notably, there were many micro-calcifications within the rotator cuff causing an inflammatory reaction. These micro-calcifications are not visible on X-ray and can only be detected by high-resolution ultrasound. Ultimately, the patient was diagnosed with frozen shoulder caused by persistent inflammation from micro-calcifications. The treatments the patient had received until now were only injections (steroid) and prolotherapy (ligament-strengthening injections). What was unfortunate was that the patient had no ligament damage, yet was receiving prolotherapy for frozen shoulder treatment. While prolotherapy is sometimes used for adhesive capsulitis, for patients like this one with no ligament damage, it was simply a waste of time and money. I remember feeling frustrated thinking that with just a bit more careful diagnosis, the patient would not have received this meaningless treatment. What I prescribed for this patient's frozen shoulder treatment was hydrodilatation, shockwave therapy, and rehabilitation. Hydrodilatation involves injecting medication into the joint capsule to break up adhesions, restore range of motion, and reduce inflammation. Shockwave therapy can treat the underlying cause of frozen shoulder by eliminating micro-calcifications. Additionally, rehabilitation exercises were prescribed to stabilize the scapula, restore glenohumeral joint range of motion, and recover thoracic spine and periscapular muscle function.
As you watch the ultrasound video, you can observe the joint capsule gradually expanding. When a medication that breaks up joint capsule adhesions is precisely injected into the capsule under ultrasound guidance, the capsule expands, helping relieve symptoms and restore range of motion.

This photo was taken one month into frozen shoulder treatment. The pain had almost completely resolved, and the range of motion had significantly improved. However, because recovery was still incomplete and physical examination showed residual capsule adhesion, a second hydrodilatation treatment was performed. From this point on, treatment continued with rehabilitation only.

At the two-month mark, the range of motion had recovered to nearly match the opposite side. From this point, only rehabilitation treatment continued.

At three months, the patient achieved complete recovery of range of motion and was free of pain. Some people believe adhesive capsulitis is a self-healing condition that does not require hospital treatment, but cases where symptoms worsen rather than improve on their own are more common. If you have frozen shoulder, rather than leaving it alone hoping for natural recovery, it is better to seek appropriate medical treatment and rehabilitation when symptoms are still mild. And to effectively treat frozen shoulder, you must find the exact cause and address it, while simultaneously providing specialized treatment (hydrodilatation, rehabilitation, etc.) for the capsule adhesion and pain.
